Pharmacotherapeutic group: Drugs used in diabetes, insulins and analogues for injection, long-acting.
ATC Code: A10A E04.
Pharmacology: Pharmacodynamics: Mechanism of action: The primary activity of insulin, including insulin glargine, is regulation of glucose metabolism. Insulin and its analogues lower blood glucose levels by stimulating peripheral glucose uptake, especially by skeletal muscle and fat, and by inhibiting hepatic glucose production. Insulin inhibits lipolysis in the adipocyte, inhibits proteolysis and enhances protein synthesis.
Pharmacodynamic effects: Insulin glargine is a human insulin analogue designed to have a low solubility at neutral pH. At pH 4, insulin glargine is completely soluble. After injection into the subcutaneous tissue, the acidic solution is neutralised leading to formation of a precipitate from which small amounts of insulin glargine are continuously released.
As observed in euglycaemic clamp studies in patients with type 1 diabetes, the glucose lowering effect of Lantus XR was more stable and prolonged in comparison with insulin glargine 100 units/ml after subcutaneous injection. The figure as follows shows results from a cross-over study in 18 patients with type 1 diabetes conducted for a maximum of 36 hours after injection. The effect of Lantus XR was beyond 24 hours (up to 36 hours) at clinically relevant doses.
The more sustained release of insulin glargine from the Lantus XR precipitate compared to insulin glargine 100 units/ml is attributable to the reduction of the injection volume by two thirds that results in a smaller precipitate surface area. (See figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Insulin glargine is metabolised into 2 active metabolites M1 and M2 (see Pharmacokinetics as follows).
Insulin receptor binding:
In vitro studies indicate that the affinity of insulin glargine and its metabolites M1 and M2 for the human insulin receptor is similar to the one of human insulin.
IGF-1 receptor binding: The affinity of insulin glargine for the human IGF-1 receptor is approximately 5 to 8-fold greater than that of human insulin (but approximately 70 to 80-fold lower than the one of IGF-1), whereas M1 and M2 bind the IGF-1 receptor with slightly lower affinity compared to human insulin.
The total therapeutic insulin concentration (insulin glargine and its metabolites) found in type 1 diabetic patients was markedly lower than what would be required for a half maximal occupation of the IGF-1 receptor and the subsequent activation of the mitogenic-proliferative pathway initiated by the IGF-1 receptor. Physiological concentrations of endogenous IGF-1 may activate the mitogenic-proliferative pathway; however, the therapeutic concentrations found in insulin therapy, including in Lantus XR therapy, are considerably lower than the pharmacological concentrations required to activate the IGF-1 pathway.
In a clinical pharmacology study, intravenous insulin glargine and human insulin have been shown to be equipotent when given at the same doses.
As with all insulins, the time course of action of insulin glargine may be affected by physical activity and other variables.
Clinical efficacy and safety: The overall efficacy and safety of Lantus XR (insulin glargine 300 units/ml) once-daily on glycaemic control was compared to that of once-daily insulin glargine 100 units/ml in open-label, randomised, active-control, parallel studies of up to 26 weeks of duration, including 546 patients with type 1 diabetes mellitus and 2,474 patients with type 2 diabetes mellitus (Table 1 and 2). Results from all clinical trials with Lantus XR indicated that reductions in HbA1c from baseline to end of trial were non-inferior to insulin glargine 100 units/ml. Plasma glucose reductions at the end of the trial with Lantus XR were similar to insulin glargine 100 units/ml with a more gradual reduction during the titration period with Lantus XR. Glycaemic control was similar when Lantus XR was administered once daily in the morning or in the evening. Improvement in HbA1C was not affected by, gender, ethnicity, age, diabetes duration (<10 years and ≥10 years), HbA1c value at baseline (<8% or ≥8%) or baseline body mass index (BMI).
At the end of these treat-to-target trials, depending on the patient population and concomitant therapy, a 10-18% higher dose was observed in the Lantus XR group than in the comparator group (Table 1 and 2).
Results from clinical trials demonstrated that the incidence of confirmed hypoglycaemia (at any time of the day and nocturnal) was lower in patients treated with Lantus XR compared to insulin glargine 100 units/ml-treated patients, in patients with type 2 diabetes treated in combination with either non-insulin anti-hyperglycaemic medicinal product or mealtime insulin. The superiority of Lantus XR over insulin glargine 100 units/ml in lowering the risk of confirmed nocturnal hypoglycemia was shown in patients with type 2 diabetes treated with basal insulin in combination with either non-insulin anti-hyperglycaemic medicinal product (18% risk reduction) or mealtime insulin (21% risk reduction) during the period from week 9 to end of study period. Overall, these effects on hypoglycaemia risk were consistently observed whatever the age, gender, BMI and duration of diabetes (<10 years and ≥10 years) in Lantus XR-treated patients compared to insulin glargine 100 units/ml-treated patients.
In patients with type 1 diabetes, the incidence of hypoglycaemia was similar in patients treated with Lantus XR compared to insulin glargine 100 units/ml-treated patients (Table 3). (See Tables 1, 2 and 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Flexibility in dosing time: The safety and efficacy of Lantus XR administered with a fixed or flexible dosing time were also evaluated in 2 randomized, open-label clinical studies for 3 months. Type 2 diabetic patients (n=194) received Lantus XR once daily in the evening, either at the same time of the day (fixed time of administration) or within 3 hours before or after the usual time of administration (flexible dosing time). Administration with a flexible dosing time had no effect on glycaemic control and the incidence of hypoglycaemia.
Antibodies: Results from studies comparing Lantus XR and insulin glargine 100 units/ml did not indicate any difference in term of development of anti-insulin antibodies, on efficacy, safety or dose of basal insulin between Lantus XR and insulin glargine 100 units/ml.
Body weight: Mean change in body weight of less than 1 kg at the end of the 6-month period was observed in Lantus XR-treated patients (see Table 1 and 2).
Results from a study on progression of diabetic retinopathy: Effects of insulin glargine 100 units/ml (once daily) on diabetic retinopathy were evaluated in an open-label 5 year NPH-controlled study (NPH given bid) in 1024 type 2 diabetic patients in which progression of retinopathy by 3 or more steps on the Early Treatment Diabetic Retinopathy Study (ETDRS) scale was investigated by fundus photography. No significant difference was seen in the progression of diabetic retinopathy when insulin glargine 100 units/ml was compared to NPH insulin.
Long term efficacy and safety outcome study: The ORIGIN (Outcome Reduction with Initial Glargine INtervention) study was a multicenter, randomized, 2x2 factorial design study conducted in 12,537 participants at high cardiovascular (CV) risk with impaired fasting glucose (IFG) or impaired glucose tolerance (IGT) (12% of participants) or type 2 diabetes mellitus (treated with ≤1 antidiabetic oral agent) (88% of participants). Participants were randomized (1:1) to receive insulin glargine 100 units/ml (n=6264), titrated to reach FPG ≤95 mg/dl (5.3 mM), or standard care (n=6273). The first co-primary efficacy outcome was the time to the first occurrence of CV death, nonfatal myocardial infarction (MI), or nonfatal stroke, and the second co-primary efficacy outcome was the time to the first occurrence of any of the first co-primary events, or revascularisation procedure (coronary, carotid, or peripheral), or hospitalisation for heart failure.
Secondary endpoints included all-cause mortality and a composite microvascular outcome.
Insulin glargine 100 units/ml did not alter the relative risk for CV disease and CV mortality when compared to standard of care. There were no differences between insulin glargine and standard care for the two co-primary outcomes; for any component endpoint comprising these outcomes; for all-cause mortality; or for the composite microvascular outcome. Mean dose of insulin glargine 100 units/ml by study end was 0.42 U/kg. At baseline, participants had a median HbA1c value of 6.4% and median on-treatment HbA1c values ranged from 5.9 to 6.4% in the insulin glargine 100 units/ml group, and 6.2% to 6.6% in the standard care group throughout the duration of follow-up.
The rates of severe hypoglycaemia (affected participants per 100 participant years of exposure) were 1.05 for insulin glargine 100 units/ml and 0.30 for standard care group and the rates of confirmed non-severe hypoglycaemia were 7.71 for insulin glargine 100 units/ml and 2.44 for standard care group. Over the course of this 6-year study, 42% of the insulin glargine 100 units/ml group did not experience any hypoglycaemia.
At the last on-treatment visit, there was a mean increase in body weight from baseline of 1.4 kg in the insulin glargine 100 units/ml group and a mean decrease of 0.8 kg in the standard care group.
Pediatric population: The efficacy and safety of Lantus XR have been studied in a 1:1 randomized controlled open label clinical trial in children and adolescents with type 1 diabetes mellitus for a period of 26 weeks (n=463). Patients in the Lantus XR arm included 73 children aged <12 years and 160 children aged ≥12 years. Lantus XR dosed once daily showed similar reduction in HbA1c and FPG from baseline to week 26 compared to insulin glargine 100 units/mL.
The dose-response analysis showed that following the initial titration phase, the body weight adjusted doses in pediatric patients are higher than in adult patients at steady state.
Overall the incidence of hypoglycaemia in patients in any category was similar in both treatment groups, with 97.9% of patients in the Lantus XR group and 98.2% in the insulin glargine 100 units/mL group reporting at least one event. Similarly, nocturnal hypoglycaemia was comparable in the Lantus XR and insulin glargine 100 units/mL treatment groups. The percentage of patients reporting severe hypoglycaemia was lower in patients in the Lantus XR group as compared to patients in the insulin glargine 100 units/mL group, 6% and 8.8% respectively. The percentage of patients with hyperglycaemic episodes with ketosis was lower for Lantus XR versus insulin glargine 100 units/mL, 6.4% and 11.8%, respectively. No safety issues were identified with Lantus XR with respect to adverse events and standard safety parameters. Antibody development was sparse and had no clinical impact. Efficacy and safety data for paediatric patients with type 2 diabetes mellitus have been extrapolated from data for adolescent and adult patients with type 1 diabetes mellitus and adult patients with type 2 diabetes mellitus. Results support the use of Lantus XR in paediatric patients with type 2 diabetes mellitus.
Pharmacokinetics: Absorption and distribution: In healthy subjects and diabetic patients, insulin serum concentrations indicated a slower and more prolonged absorption resulting in a flatter time-concentration profile after subcutaneous injection of Lantus XR in comparison to insulin glargine 100 units/ml.
Pharmacokinetic profiles were consistent with the pharmacodynamic activity of Lantus XR.
Steady state level within the therapeutic range is reached after 3-4 days of daily Lantus XR administration.
After subcutaneous injection of Lantus XR, the intra-subject variability, defined as the coefficient of variation for the insulin exposure during 24 hours was low at steady state (17.4%).
Biotransformation: After subcutaneous injection of insulin glargine, insulin glargine is rapidly metabolized at the carboxyl terminus of the Beta chain with formation of two active metabolites M1 (21A-Gly-insulin) and M2 (21A-Gly-des-30B-Thr-insulin). In plasma, the principal circulating compound is the metabolite M1. The exposure to M1 increases with the administered dose of insulin glargine. The pharmacokinetic and pharmacodynamic findings indicate that the effect of the subcutaneous injection with insulin glargine is principally based on exposure to M1. Insulin glargine and the metabolite M2 were not detectable in the vast majority of subjects and, when they were detectable their concentration was independent of the administered dose and formulation of insulin glargine.
Elimination: When given intravenously the elimination half-life of insulin glargine and human insulin were comparable.
The half-life after subcutaneous administration of Lantus XR is determined by the rate of absorption from the subcutaneous tissue. The half-life of Lantus XR after subcutaneous injection is 18-19 hours independent of dose.
Paediatric population: Population pharmacokinetic analysis was conducted for Lantus XR based on concentration data of its main metabolite M1 using data from 75 pediatric subjects (6 to <18 years of age) with type 1 diabetes. Body weight affects the clearance of Lantus XR in a nonlinear way. As a consequence, exposure (AUC) in pediatric patients is slightly lower as compared to adult patients when receiving the same body weight adjusted dose.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image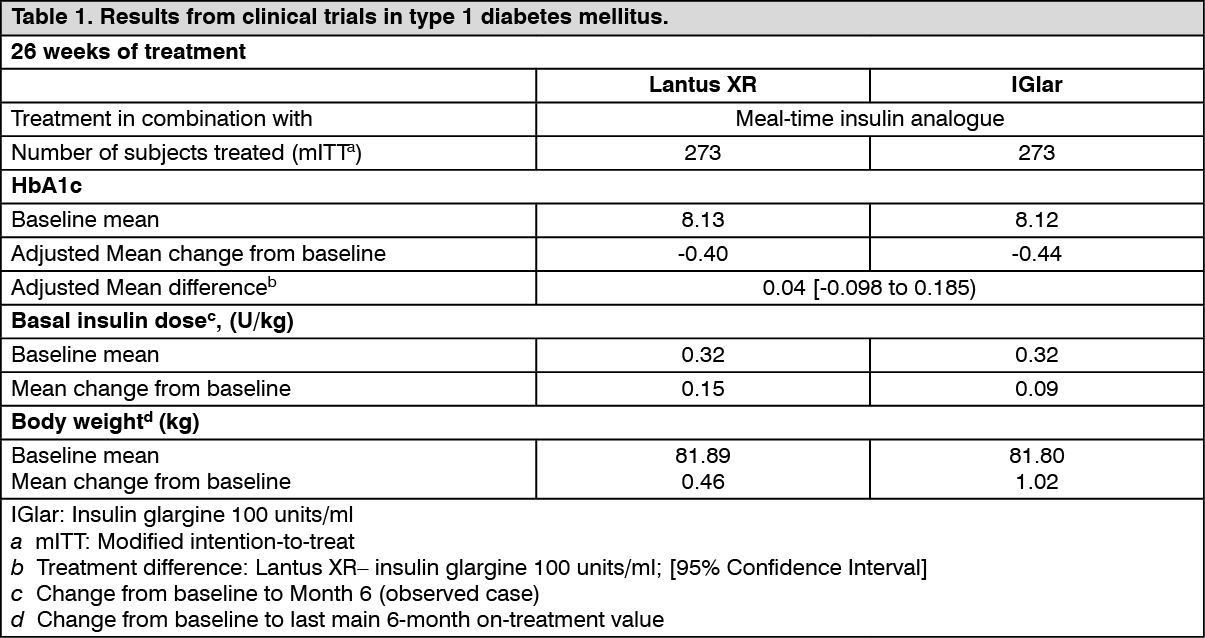 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image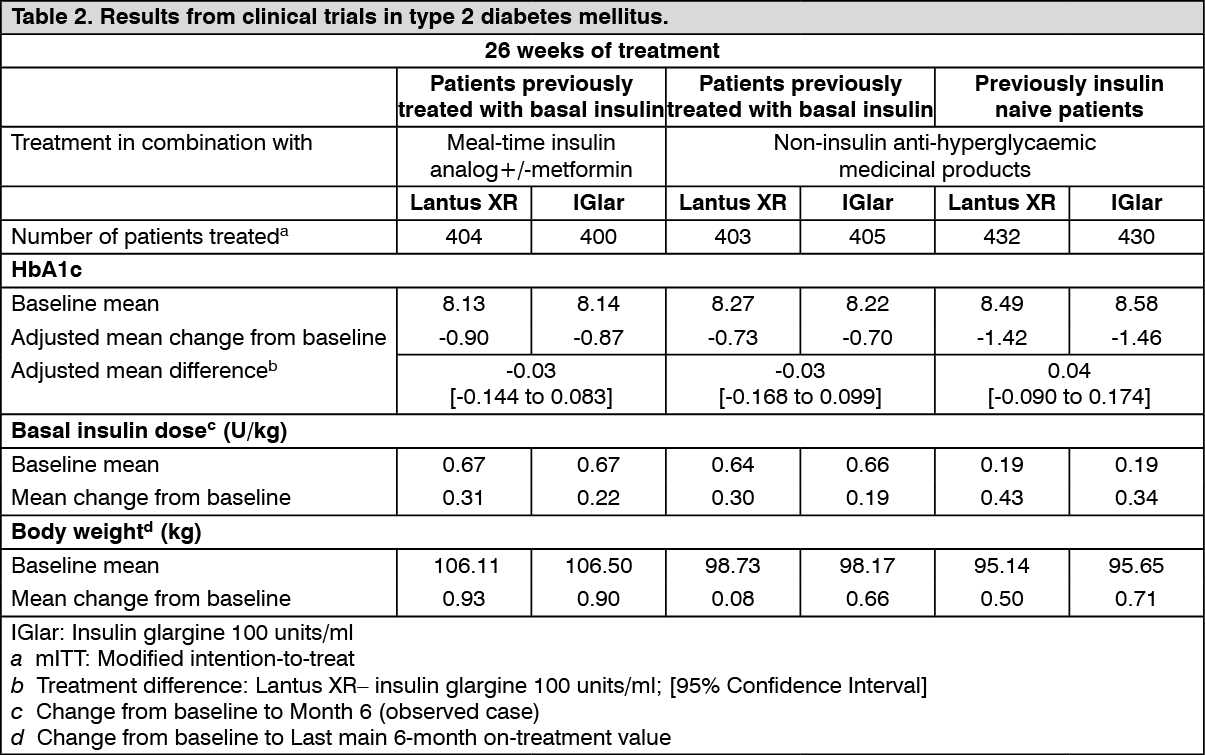 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image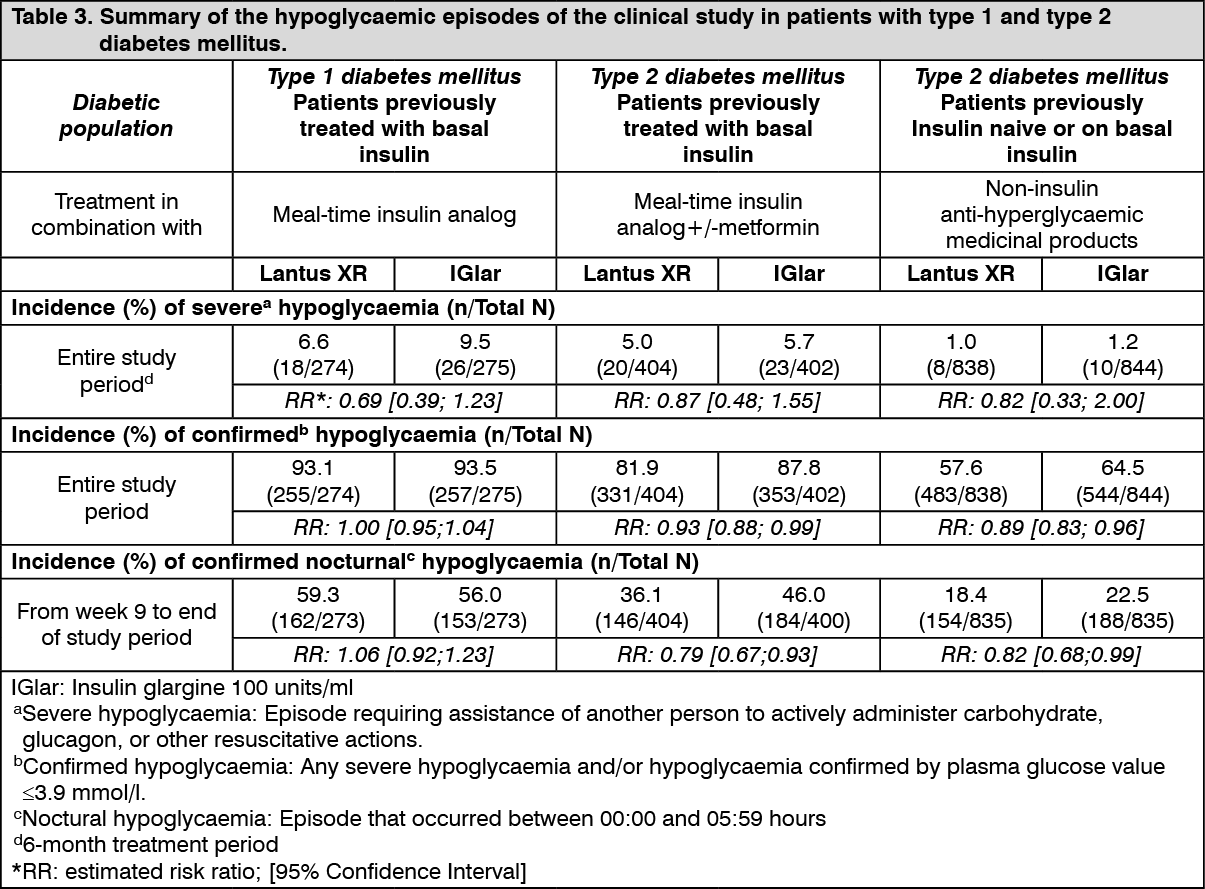 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
